According to the PSA team, the Covid-19 situation and the company's response to it did not contribute to the incident. West Bollsta was on the Polmak prospect, well 7221/4-1, in the southern Barents Sea when the incident occurred.

Design phase and ordering/installation of the equipment
The PSA team reviewed the governing documents related to the equipment and personnel involved, as well as operational procedures and other documentation. The HTO investigative method was used as the basis for the work of the PSA group.
Preparations for operation in Norway before the incident
Seadrill's investigation and further testing of the relevant onshore equipment was followed up from November 2020 until the Seadrill report was received by PSA on 11 January 2021.
The actual incident
Figure 3: Joint lying on the floor of the drill and on top of the spider after the incident. Figure 4: How the arms of the gorilla, placed on the catwalk to handle the joints, bent due to the weight of the joint after the incident.
After the incident
Time line
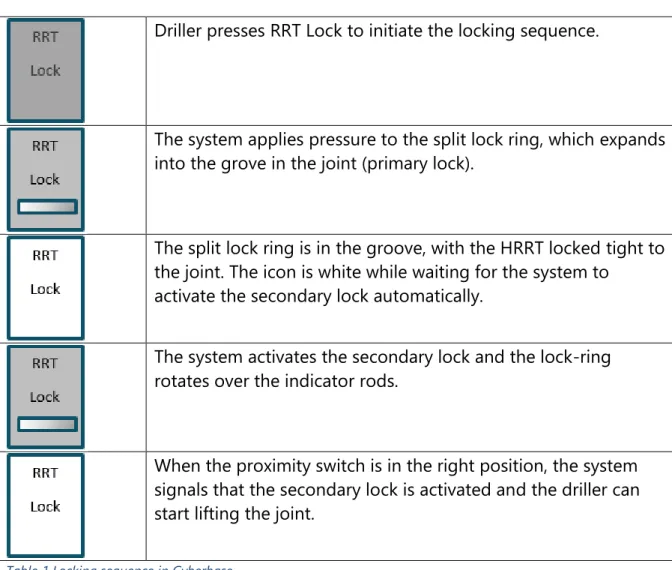
The split lock ring is in the groove, with the HRRT firmly locked into the joint. He was not supposed to see this light when the HRRT was locked in the joint.
Technical set-up for riser handling on West Bollsta
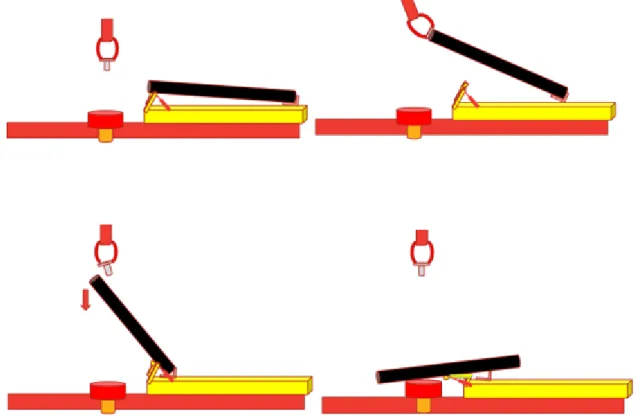
The HRRT and insertion in a joint
Verification of locking
HRRT control system
Third-party certificates and verifications
Operational and organisational conditions the drill floor
Personnel with roles related to riser handling
To ensure that staff can fulfill their role as a barrier or part thereof, this must be clearly defined and understood for the different work assignments. Seadrill had a step-by-step procedure (Run BOP, doc. no. SSP87-0060) for riser handling, which defined roles and responsibilities among drilling department personnel. Verification of the secondary lock had to be carried out by personnel fairly close to the equipment on deck.
Point 14 of the step-by-step procedure required the assistant driller or subsea supervisor to verify and then confirm to the driller that the hydraulic primary and secondary locks were in place and active. During the investigation it emerged that, contrary to procedure, the division of tasks, roles and responsibilities on the drill floor was normally not agreed before the start of an operation.
Communication and information on riser handling
The system applies pressure to the split lock ring, which expands into the groove in the joint (primary lock). When the proximity switch is in the correct position, the system signals that the secondary interlock is activated and the driller can begin lifting the joint. After converting from manual to hydraulic secondary locking, the locking mechanism was designed so that everything can be controlled hydraulically after the HRRT is properly positioned in the joint.
On the other hand, the drill's display in the simulator was more or less identical to the one on board. If the HRRT were not fully inserted, the profile of the split retaining ring would be clamped to the connecting wall and therefore not engage the groove therein. This must have occurred between the time the roustabout saw the HRRT inserted into the joint as it entered the drill floor and the time they saw the secondary retaining ring rotate during the actual verification.
The user manual for the HRRT was flawed, as the instrument in the manual did not match the one used on board. In the team's opinion, the driller was the operator of the HRRT, while the roustabout, who confirmed that it was tightly locked to the joint, had the banker role. A review of the system revealed that it did not include SDLAs in general, or the HRRT involved in the incident in particular.
Training and expertise
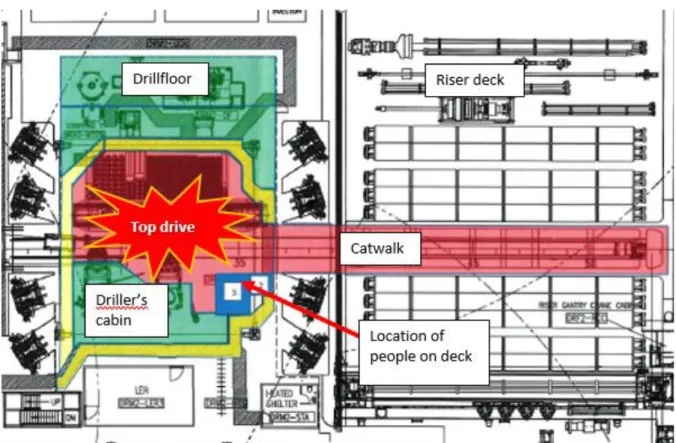
Actual consequence
The puck landed in the red zone while two people were on the practice floor near the strike zone. In the fall, the joint damaged the V-door of the tube deck and several of them.
Potential consequences
Theory 1: locking mechanism fully engaged with the joint
It emerged from the investigation that both the user manual and procedures lacked a precise description of the locking mechanism and how the staff on board could check that it was engaged. During the test, the HRRT was retracted to create a 20 mm gap between the upper spacer block and the upper edge of the assembly. Requirements for lifting equipment are specified in section 69 of the building regulations on lifting equipment and lifting equipment.
This does not appear in the documentation the PSA team received, nor was it indicated on the HRRT. A number of the observations in this research report were reported to Seadrill in the form of non-conformities and areas for improvement following previous audits and investigations by the PSA. This meant that the description of how staff were supposed to verify the HRRT's lockout was inaccurate.
The PSA team learned that the exercise was for one of the roustabouts to perform. Articles 24, paragraph 2 of the activities regulations on procedures, and article 92 on lifting operations, see the guidelines that refer to Norsok R-003N on safe use of lifting equipment. Risk analysis prior to lifting the load could not provide an integrated and nuanced picture of the risk associated with lifting the drill floor.
The person to verify with the driller that the HRRT was locked tight to the joint had not been determined prior to the lift. The design of the HRRT meant that the driller could not rely on the screen report that it was locked.
Theory 2: locking mechanism partly engaged with the joint
Theory 3: locking mechanism not engaged with the joint
The verification itself is described in sections 5.1.1 and 5.1.2 on HRRT and assembly in an assembly and verification of locking, respectively, where it has also emerged that there are technical deficiencies in the system for reporting to Cyberbase that the system is locked and promises. can begin. When the locking sequence started, tests on land showed that even a slight movement in the secondary locking ring could give an inaccurate signal to Cyberbase that the tool was locked. Tests also showed that this could occur in cases where the HRRT was not adequately inserted into the riser.
As a result, the piston would also not be able to move down the split washer and the indicator rods would not be able to drop into the HRRT and be locked in place by the secondary washer. This small movement may be enough for the proximity switch to indicate to Cyberbase that the HRRT is locked. It appeared from interviews that roustabouts who confirmed a successful lockout in the field saw the secondary locking ring move and assumed the operation was successful.
Field testing shows that if the HRRT were plugged into the joint and not hanging from the top drive, it would have an angle between 2 and 2.2. Under these conditions, the HRRT failed to lock onto the joint during the land test. This is shown in the diagram and photo below, taken from the Sub Sea Services test report.
Underlying causes
Many serious incidents have occurred on both fixed and mobile facilities with material handling equipment for use in drilling operations on the drill floor. The PSA's investigation into the falling riser joint on West Bollsta saw that many of the direct and underlying causes identified in earlier incidents with this type of equipment on the NCS were also found in this case. To operate on the NCS, drilling facilities such as West Bollsta must have an AoC as specified in section 25 of the framework regulations.
Article 1, letter a of the Facilities Regulations notes that Article 3 of the Framework Regulations does not apply to provisions relating to drilling and process equipment. When it comes to the relevant lifting equipment involved in the incident, an RRT of this type is included in Norsok R-002 and defined as an SDLA with specific requirements. It also provides guidance on how lifting equipment – including equipment classified as an SDLA – should be monitored both technically and operationally.
Seadrill has chosen to apply Norsok R-003N for the safe use of lifting equipment and Norsok R-002 on lifting equipment as requirements in its management system. Compliance (AoC)/IADC HSE Case, rev 1 Seadrill confirms its compliance with those parts of the PSA regulations that the investigation team applied when evaluating its observations. Points for improvement: these relate to observations where deficiencies are noted, but insufficient information is available to prove a breach of the regulations.
Nonconformities
- Design of lifting equipment
- Correction of earlier nonconformities and orders
- Continuous improvement
- Management system for lifting operations
- Procedures for executing work
- Organisation and exercise of roles and responsibilities
- Risk assessments and measures
- Maintenance of lifting equipment
- Expertise
Part of the evidence for this non-compliance was the inadequate follow-up of the competent audit findings. The next section of the procedure on making double connections (Make a double connection from riser to BOP) specified that the driller should receive a signal on his screen and that the drill floor personnel should check and confirm that the tool is properly was stuck. to the joint. It also emerged that even at the time of the investigation, Seadrill had no personnel in the land organization with responsibility and expertise in crane operations and lifting equipment.
The TBRA for the lifting of the joint carried out shortly before the incident identified the following risk in the "On the day risk" box: "First time in operation". The TBRA for lifting the load was carried out without the driller, although the latter led the lift and acted as operator of the top drive that lifted the load. Personnel on board were aware of flaws in the step-by-step procedure for the task and in the user manual for the equipment.
Sections 5, 13 and 17 of the regulations on the management of obstacles, with guidelines, on work processes and on risk analyses. Interviewees also confirmed that no specific training was provided for this type of equipment, except that some crew members were trained to use it at West Bollsta before the facility became operational. According to the PSA Group, the incident can be attributed to an interaction between technical, organizational and operational factors.
However, it has not been able to identify a clear cause or confirm one of the theories outlined in Chapter 7. In the PSA team's opinion, the observations in Seadrill's report largely coincide with those made in its investigation report.